9 Reasons why we need to open NOW!
In a nutshell we should open up NOW and stay open, unless something changes dramatically. The Covid19 risk is within the same risk level as historical influenza outbreaks that did NOT result in economic shutdown. The number of studies that debunk the 3.5% and 7% death rates are overwhelming.
Last updated: 5/22/2020
One other key thing. Infection testing is less important that anti-body testing. If you have the anti-bodies you cant be seriously infected with the same virus strain again.
Reason 1: The Death Rate is a LOT lower than reported.
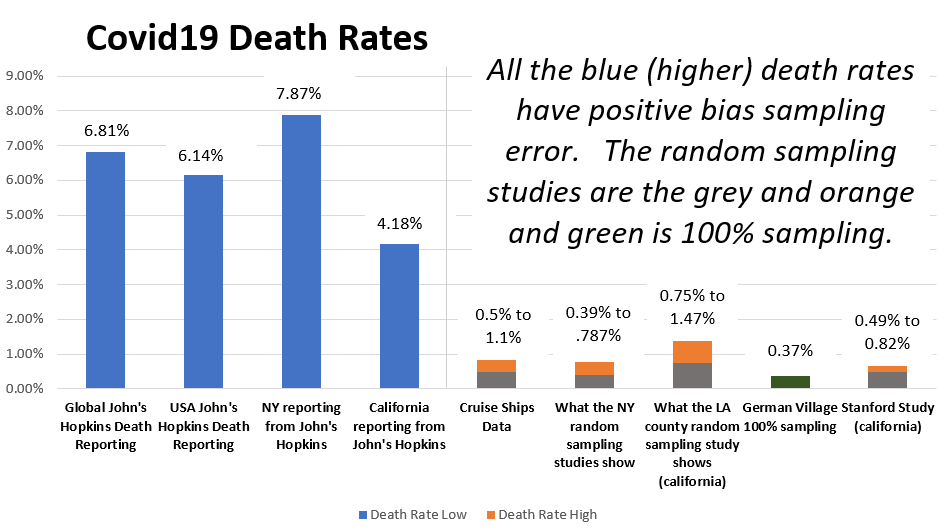
The number reported is correct except no one understands that it is knowingly wrong because of sample error. The blue columns are what are regularly reported on TV. The real numbers are 5 to 20x lower
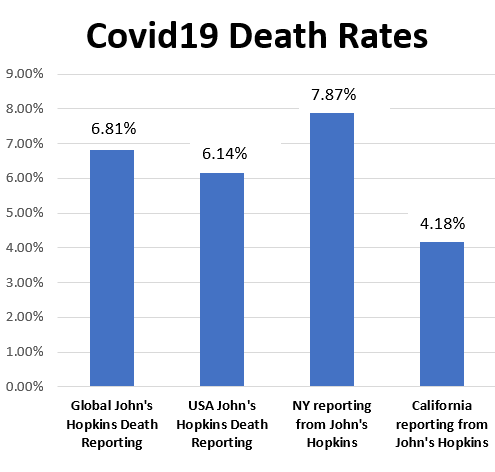
The ACTUAL random samples (below) are in grey and orange. The random or 100% sampling death rates are between 0.39% and 1.47% not the 3.5% or 7% being reported. The German study was the lowest of all and had 100% sampling.
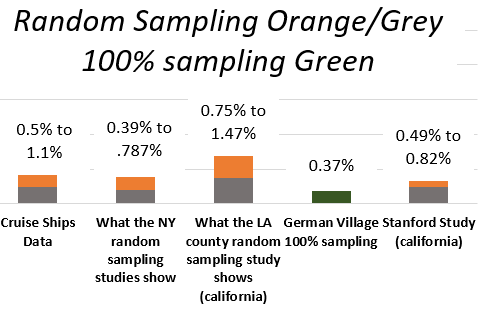
The difference between the John’s Hopkins numbers and these studies is purely sampling bias or “error”. The blue represents a sampling of tested sick people. The orange and grey represent a sampling of an entire group of people (those sick and those who don’t appear to be sick).
Recently the “death rate” fell from 7% to 6.01% – that is highly unlikely, and indicates wider testing not decreased lethality.
What is Sampling Bias?
Nearly all the currently reported data is misleading. A simple example of sampling bias: Only sample the fish in a grocery store. You measure size and type. The sample shows all the fish are fairly large, uniform and of limited number of species. If I go out and randomly catch fish in rivers, lakes and oceans, the size and types of fish vary widely. (sample bias vs random sampling)
What is Omission Bias?
Omission bias is reporting a fact but skipping related facts. Example: News headlines say “infection rates spiking!” but they fail to report real data like hospitalization utilization compared to normal hospitalization rates and death rates compared to NORMAL death rates. Infections alone don’t really mean anything.
Another omission is that the widely reported information is ONLY for those sampled (it is not random sampling). We rarely here about random sampling statistics.
Read more about sampling bias
- https://en.wikipedia.org/wiki/Sampling_bias
- https://towardsdatascience.com/were-21-of-new-york-city-residents-really-infected-with-covid-19-aab6ebefda0 I don’t entirely agree with his presumptions re: covid19 but his descriptions of various BIAS types is 100% accurate.
Reason 2: Most Hospitals are Not Overloaded
We were told we were trying to flatten the curve. Remember this graph?

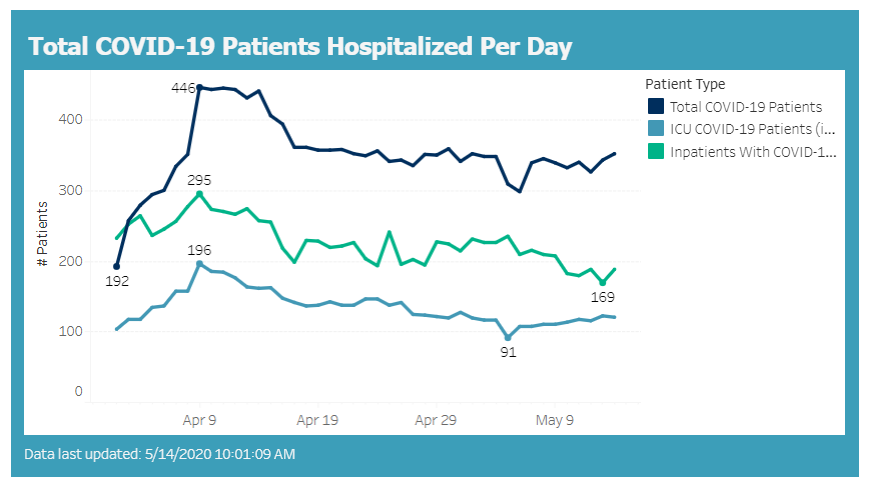
In this example above, we all get Covid19 but we get it slow enough that we didn’t overwhelm healthcare. We didn’t overwhelm the system. We flattened it completely. In fact we have created a situation where it is TOO flat. As an example in Wisconsin the ICU load was less than 10% NORMAL utilization and 7.6% of max utilization.
With this very low utilization, the hospitals will go bankrupt quickly, so unless the goal was to bankrupt hospitals – we need to change our behavior. Source: https://www.wha.org/COVID19Update
Another way to look at the numbers

Image: Wisconsin ICU Bed Utilization
** does not include temporary military hospitals which are EMPTY.
Wisconsin regularly reported increases in hospitalization. But the fact is that hospitals in Wisconsin were regularly below 20% utilization from April through May 2020. Nationwide over 256 hospitals had to lay off staff. There was not a huge spike nationwide, there were spikes in specific locations (just like a bad flu season). https://www.beckershospitalreview.com/finance/49-hospitals-furloughing-workers-in-response-to-covid-19.html.
Reason 3: Only 15% or less of us are at risk
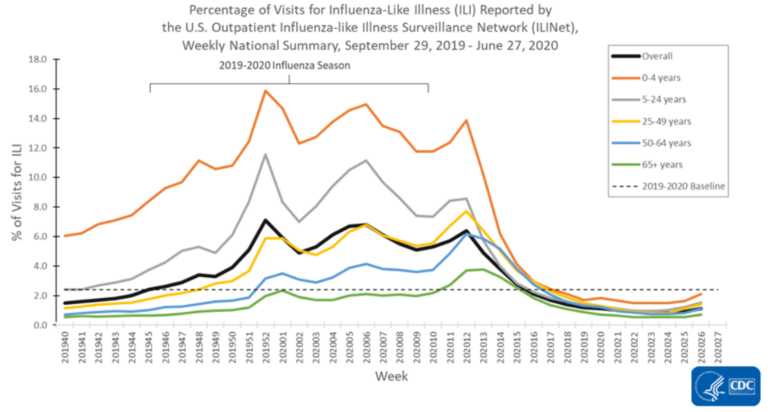
We were told, we are ALL at risk! We are in this together. A half truth. Yes, everyone is at risk. We are at risk of dying from pretty much everything and there is a 100% chance we will all die. The facts are that the risk is high for elderly and people with pre-existing conditions, and very low for everyone else (see graphs)
Remember, even these numbers are biased because they are not random sampling of the population. This is ONLY those who were infected or suspected of being infected.

We should be focusing our limited resources on the 15% of the population that is at risk, not the 85% of us that are at low or very low risk.

Reason 4: Yes people are dying, but not a lot more than normal
Cold hard math, unpleasant, uncomfortable thoughts. The numbers of people dying are not significantly higher than normal. It feels like this cant be true. The news says its unprecedented but the numbers don’t lie.
Here is a graph from CDC of normal (orange line) and actual deaths blue. Note only two spikes in 2018 and one in 2020 – and note not hugely different. For historical comparison we had influeza spikes that were equal or higher per 100k and we didn’t put 22 mil into unemployment and bankrupt 4% to 12% of small businesses.

If the .39% death rate is true that is 2.7 times as dangerous as normal flu (like the 1998 flu season).
Image: CDC Normal Death Rates
https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm. https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htm
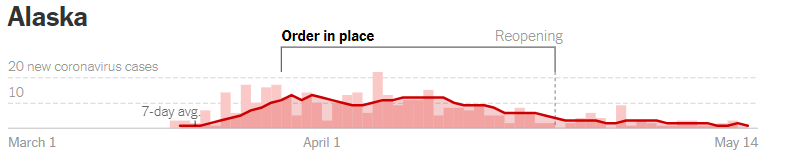
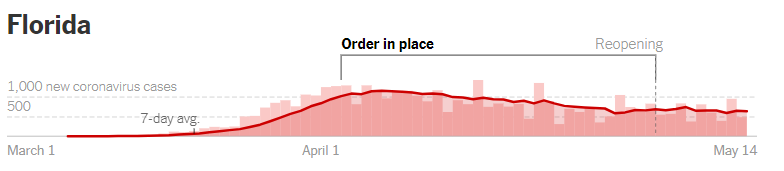
Reason 5: Big Events haven’t resulted in increased death
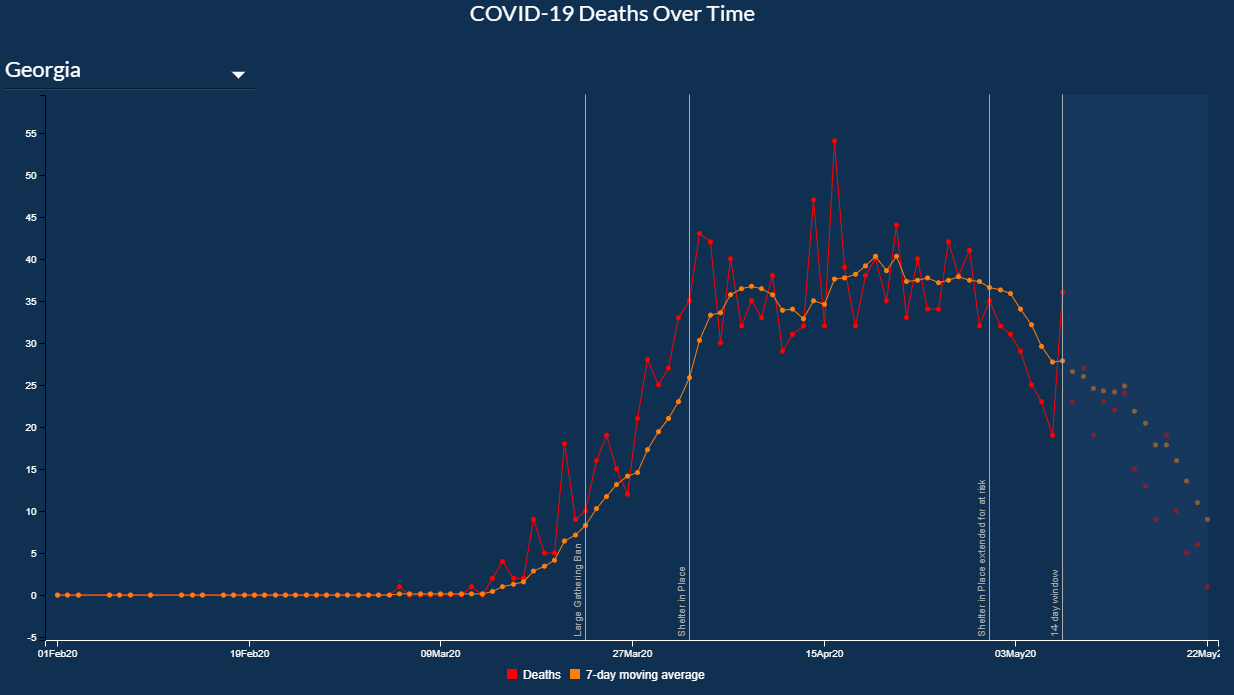
Big events such as: elections, rallies and reopening entire states have had no impact on death rates. Georgia re-opened April 24th.

On May 22nd the predicted 1000s of Georgia deaths didn’t materialize. The graph below confirms the graph above. At minimum, there is no increase in deaths, even with the state being “open”. 28 days later there is a downward trend in deaths (or at least no significant increase).
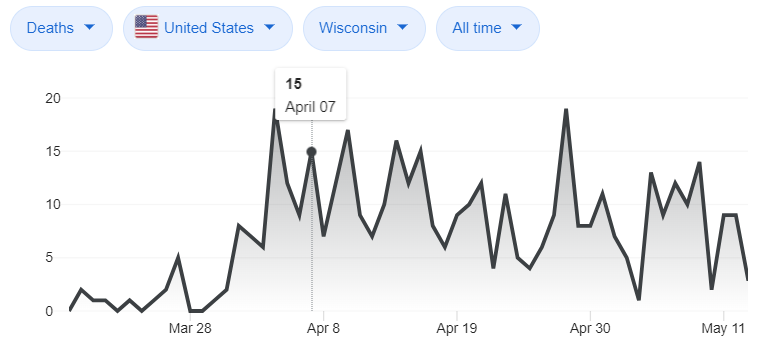
On April 7th Wisconsin had an in person election with 300,000+ people participating. Wisconsin had a rally with 3000+ people (mostly without masks) on April 24th, and 28 days later there is no big spike in deaths. The predicted 1000s of deaths in Wisconsin didn’t materialize.
The following are other examples of decreasing or stable trends after reopening. See CNN link for updated data
Reason 6: Staying inside will not stop the virus.
The idea that staying inside will “stop the virus” is purely wishful thinking. WHO, CDC and all other agencies all expected us to get the virus. The only goal was to reduce the number of people infected at one time. If we stay inside more all we do is SLOW the spread, we dont STOP the spread.
You may have seen a graph on social media called “flattening the curve.” That graph shows a tall, narrow curve and a short, wide curve. Through the graph is a line that shows how many sick people U.S. hospitals can treat. The tall curve goes above the line. That means too many people are sick at one time: We won’t have enough hospital beds for all the people who will need treatment. The flatter curve shows what happens if the spread of the virus slows down. The same number of people may get sick, but the infections happen over a longer span of time, so hospitals can treat everyone.
https://www.webmd.com/lung/qa/what-is-flattening-the-curve
The CDC, WHO and other medical agencies never said staying home would “stop the virus”. Staying home only delays things – it will not stop Covid19.
Also, we need real herd immunity so we can protect those at most risk. Thinking that hiding and still going out only to Walmart or Costco will somehow “protect us” is not realistic.
Reason 7: Staying locked down hurts and kills people
We have 22million+ people already unemployed. In a good year we have 45,000 suicides – the economic crash is NOT going to help that number, and increases in suicides are reported widely. Decreases in GDP will result in decreased govt revenue which will result in decreased govt support for those in need of help. LOST REVENUE WILL RISK LIVES.
Related articles
- https://www.reuters.com/investigates/special-report/health-coronavirus-usa-cost/
- https://loudwire.com/suicide-rates-could-increase-covid-19-how-seek-help/
The UN is noting that worldwide famine is likely because of Covid. https://www.nbcnews.com/news/world/u-n-warns-hunger-pandemic-amid-threats-coronavirus-economic-downturn-n1189326
We are hiding at home from a virus that we will get sooner or later. We are trading higher suicides, higher poverty, loss of freedom, reduced revenue for critical services, and directly leading to famine overseas to simply put off the inevitable?
At some point we NEED to get infected. If we stick our head in the sand, this fall 2020 and winter 2021 version of Covid19 will be even worse (read about the Spanish flu if you haven’t). We need to build up immunity
Reason 8: The Vaccine won’t solve it
Even if we get a vaccine (which I hope is safe and effective). It is likely to be at most 20% effective. So we are going to see people get infected and some will die. That is a fact, that unfortunately cannot be avoided. Once we reopen (even with a vaccine) we will see increased infections and death. Likely to exceed a 100 million infections nationwide and 300,000 deaths when it is all done.
Delaying the infection is all we can do, and the WAY we are delaying now destroys our econmony which destroys our ability to help those most in need.
Reason 9: Return Choice to the People
This is our constitutional right, and the government is overstepping by taking it away. I talked with my parents who are 77 and 81. They would trade their lives to protect their children and grandchildren in a minute. I don’t want to make that trade, but I cannot lock them away either. And WE don’t have the right to take away other peoples children’s futures.
This is a serious, real dilemma. But we have been and I hope we continue to be focused on freedom, shared risk and personal responsibility. Recommending behavior and allowing the PEOPLE to decide is the only way we are going to succeed in the long run.
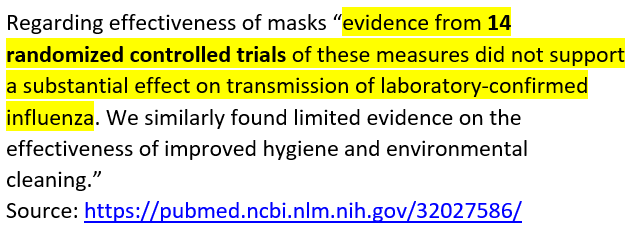
Why Masks Should Not Be Mandatory
It is ok to recommend masks, but mandating the use of masks is not supported by studies. Quite the contrary, there are numerous studies and reports that indicated low value and some limited risks with ongoing use of face mask.
Further, non-medical, home made or “cloth” masks are even less effective. Also, reuse of masks introduces other bacterial and viral risks, which have limited studies, some of which indicate secondary bacterial and secondary transmission risks.
- Failures and problems with extended facemask use https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2662657/
- Covid19 4 out 4 failure for masks: https://annals.org/aim/fullarticle/2764367/effectiveness-surgical-cotton-masks-blocking-sars-cov-2-controlled-comparison
- Risks of prolonged facemask use and retransmission https://oeh.tandfonline.com/doi/full/10.1080/15459624.2014.902954#.XsgLFGhKhPY
- Limited evidence supporting the efficacy or effectiveness of face masks to reduce influenza virus transmission. https://www.cambridge.org/core/journals/epidemiology-and-infection/article/face-masks-to-prevent-transmission-of-influenza-virus-a-systematic-review/64D368496EBDE0AFCC6639CCC9D8BC05
- Only N95 masks are significantly effective against bacterial colonization, co-colonization, viral-bacterial co-infection and dual virus infection https://www.sciencedirect.com/science/article/pii/S0091743514000322
- Masks Fail to Filter Virus in Coughing COVID-19 Patients https://www.medpagetoday.com/infectiousdisease/covid19/85814
References
- CDC Covid19 Transmission information https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/how-covid-spreads.html
- Johns Hopkins source data https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf62
- Cruise Ship source data https://www.medrxiv.org/content/10.1101/2020.03.05.20031773v2
- LA County Study: 0.5% and 1.1%. http://publichealth.lacounty.gov/phcommon/public/media/mediapubhpdetail.cfm?prid=2328&fbclid=IwAR2odNQwAchsTdMsTPW9Q4YfqLPzSreSn16imtSsKzV-eWyGm6wfK5ecv-A That estimate is 28 to 55 times higher than the 7,994 confirmed cases of COVID-19 reported to the county by the time of the study in early April.4.
- Stanford study https://www.washingtonexaminer.com/news/random-sampling-test-shows-coronavirus-more-widespread-and-less-deadly-than-previously-thought-study? fatality rate 50-85 x lower than the crude numbers would suggest
- New York Random Sampling https://www.nytimes.com/2020/04/23/nyregion/coronavirus-antibodies-test-ny.html
- German Example: (14% infection rate) and a COVID-19 infection fatality rate of about 0.37 percent (and could be lower).
https://reason.com/2020/04/09/preliminary-german-study-shows-a-covid-19-infection-fatality-rate-of-about-0-4-percent/
First Published May 15th 2020.